

As a Paediatrics Orthopaedics doctor in Bhubaneswar, one of the most frequent emergencies I encounter in my clinic is bone fractures in children. Falls from bicycles, playground injuries, sports accidents — children are active, and injuries are part of growing up. But not every parent knows how to recognise a fracture, when to seek help, or what the treatment journey looks like.
This guide is written to help parents in Bhubaneswar and across Odisha understand Paediatrics Orthopaedics fractures — what makes them unique, the types most commonly seen in children, warning signs to watch for, and the treatment options available.
Table of Contents
- Why Children’s Bones Are Different from Adults
- Common Types of Paediatric Fractures
- Signs and Symptoms Parents Should Never Ignore
- Understanding Growth Plate Injuries
- How Are Paediatric Fractures Diagnosed?
- Paediatric Fractures Treatment: What to Expect
- Recovery and Rehabilitation
- Prevention Tips for Parents
- When to Visit a Paediatrics Orthopaedics Doctor in Bhubaneswar
- Frequently Asked Questions (FAQ)
1. Why Children’s Bones Are Different from Adults
Children are not simply “small adults” when it comes to bone injuries. Their skeletal system is still developing, and this creates both advantages and vulnerabilities that are unique to paediatric patients.
Key differences include:
- Greater flexibility: Children’s bones contain more water and collagen, making them more pliable. They can bend before breaking — which is why fracture patterns like “greenstick” and “buckle” fractures are unique to children.
- Active growth plates: Also called the physis, these are areas of cartilage near the ends of long bones where growth occurs. They are structurally weaker than mature bone and are vulnerable to injury.
- Faster healing: Children’s bones have a more active blood supply and a thicker periosteum (the outer bone layer). New bone forms much faster in children than in adults.
- Remodelling capacity: Children’s bones can partially correct mild misalignment over time through a process called remodelling — something adult bones cannot do as effectively.
💡 Doctor’s Note: A fracture that would require surgery in an adult might heal perfectly with just a cast in a child. This is why paediatric fractures must always be evaluated by a specialist who understands growing bones.
2. Common Types of Paediatric Fractures
Understanding the type of fracture helps parents know what to expect from paediatric fractures treatment. Here are the most common types I see in children.
Greenstick Fracture
Named after a green twig that bends and cracks rather than snapping cleanly, a greenstick fracture breaks one side of the bone while the other side bends. These are most common in the forearm. Because children’s bones are more flexible, they absorb force differently than adult bones. Treatment usually involves casting for 3–5 weeks.

Buckle (Torus) Fracture
This is one of the most common fractures I treat as a Paediatrics Orthopaedics doctor in Bhubaneswar. It occurs when the bone compresses and buckles on itself — typically seen at the wrist after a child falls and puts out their hand to catch themselves. These are considered stable fractures and often heal well with a splint or removable brace.

Complete Fracture
The bone breaks all the way through. These are categorised further as transverse (straight across), oblique (angled), or spiral (twisting force, often from sports). Complete fractures may require casting or, in some displaced cases, surgical correction.

Comminuted Fracture
The bone shatters into multiple fragments. These are less common in children due to bone flexibility but can occur in high-impact injuries such as road accidents. Surgical intervention is more often needed.
Stress Fracture
Tiny cracks that develop from repetitive overuse rather than a single trauma. These are increasingly seen in young athletes — especially in the shin, foot, and lower back. A child who develops persistent pain during a specific activity should be evaluated promptly.
Open (Compound) Fracture
The bone pierces through the skin. This is a medical emergency requiring immediate hospital care to prevent infection and manage bone integrity.
3. Signs and Symptoms Parents Should Never Ignore
Many parents ask me: “How do I know if my child has a fracture or just a sprain?” Here are the warning signs of children’s bone fractures that should prompt an immediate visit:
Definite red flags:
- Sudden, severe pain at the injury site
- Visible deformity or unnatural bend in a limb
- Bone visible through the skin (open fracture — call emergency services immediately)
- Inability to move the affected arm or leg
- Refusal to bear weight on a leg or use an arm
- Rapid swelling and bruising around the injury
- A distinct “snap” or “pop” heard at the time of injury
- Persistent pain even at rest
In younger children and toddlers, also watch for:
- Inconsolable crying that doesn’t ease with comfort
- Refusal to move a limb entirely (called pseudoparalysis)
- Tenderness to light touch
- Crying when you try to dress or undress the child
⚠️ Warning: Never try to realign a suspected fracture at home. Immobilise the limb gently in the position found and seek medical attention immediately.
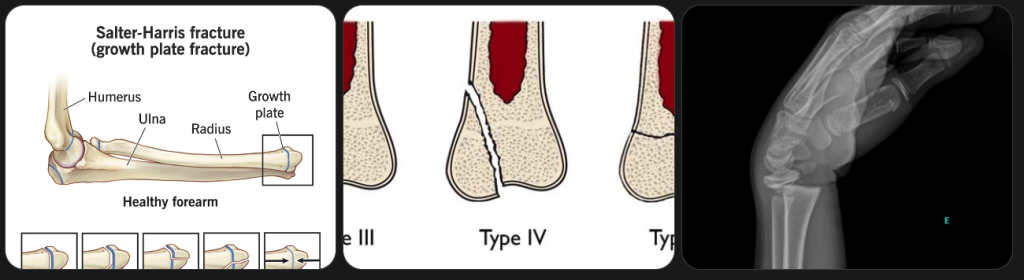
4. Understanding Growth Plate Injuries
Growth plate fractures deserve special attention. The growth plate (physis) is the area of developing cartilage at the end of long bones in children — it’s where bone length increases as your child grows. Since these plates are softer than mature bone, they are the weak link in a child’s skeletal system.
Why are they serious?
If a growth plate fracture is not treated correctly, it can disrupt the bone’s ability to grow properly — potentially leading to one limb being shorter than the other, or angulation deformities. Approximately 15–30% of all childhood fractures involve the growth plate.
The Salter-Harris classification system grades growth plate injuries from Type I (mildest) to Type V (most severe). Type I and II injuries generally heal with casting alone. Type III, IV, and V injuries may need surgical fixation to preserve growth.
Most common growth plate fracture sites in children:
- Wrist (distal radius)
- Ankle (distal fibula)
- Fingers
- Knee (distal femur — higher risk of complications)
💡 Key Message: If your child injures a joint and pain persists beyond 24–48 hours, please do not assume it is “just a sprain.” Growth plate injuries can look like sprains on initial examination. A specialist evaluation — and sometimes an MRI — is needed.
5. How Are Paediatric Fractures Diagnosed?
When you bring your child to my clinic as a best paediatrician in Bhubaneswar, the diagnostic process follows a systematic approach:
Clinical examination first: I assess the child’s pain level, check for swelling, deformity, tenderness, and test range of motion carefully.
Imaging:
- X-ray — the first-line investigation for most suspected fractures. In children, comparison X-rays of the unaffected side are sometimes taken because growth plates can be mistaken for fracture lines.
- Ultrasound — increasingly used in children to avoid radiation, especially for rib fractures and soft tissue injuries.
- MRI — the gold standard for growth plate injuries, stress fractures, and cartilage damage. No radiation involved, making it ideal for children.
- CT scan — reserved for complex fractures where detailed bone anatomy is needed for surgical planning.
6. Paediatric Fractures Treatment: What to Expect
The good news: most paediatric fractures treatment — 70 to 80% of cases — is non-surgical. Children’s natural healing capacity and remodelling ability means many fractures that would require surgery in adults can be managed conservatively.
Non-Surgical Treatment
Casting is the most common treatment. A plaster or fibreglass cast holds the bone in alignment while it heals. Depending on location and severity, casting periods range from 3 to 8 weeks. I always ensure the cast fits well and educate parents on warning signs of a cast that’s too tight (numbness, swelling, colour change of fingers or toes).
Splinting is used for less severe fractures, particularly buckle fractures of the wrist. Splints allow some swelling and can be removed for bathing (as advised).
Closed Reduction — In cases where the bone is displaced or angulated, I may need to realign the bone manually under sedation before applying the cast. This is done carefully to avoid further trauma.
Surgical Treatment
Surgery is considered when:
- The fracture is significantly displaced and cannot be held by casting
- The fracture involves the joint surface (intra-articular)
- Growth plate injuries are of higher severity (Salter-Harris III, IV, V)
- There is an open (compound) fracture
- There is neurovascular compromise (nerve or blood vessel damage)
Surgical options include:
- K-wires (Kirschner wires) — thin metal pins inserted to hold bone fragments in place. These can often be removed in the clinic after healing.
- Elastic intramedullary nailing — flexible rods passed through the bone canal for certain long-bone fractures, especially the femur and forearm.
- External fixation — metal frame applied outside the body for severe open fractures or comminuted injuries.
💬 From My Clinic: I always discuss treatment options in detail with parents before proceeding. The goal is always the most conservative approach that ensures safe, complete healing — preserving both the bone’s integrity and your child’s future growth.
7. Recovery and Rehabilitation
Children recover from fractures faster than adults — but recovery still requires patience and attention.
Timeline by age and fracture type:
- Toddlers (1–3 years): Simple fractures may heal in as little as 2–3 weeks
- School-age children (4–10 years): 3–6 weeks for most fractures
- Adolescents (11–17 years): 4–8 weeks; healing is slower as growth approaches adult rates
- Growth plate fractures: 6–12 weeks, with follow-up X-rays to confirm proper healing
During recovery:
- Follow activity restrictions strictly — premature return to activity is the most common cause of re-fracture
- Keep the cast dry and check daily for skin irritation or pressure sores
- Encourage gentle finger or toe exercises to prevent stiffness in adjacent joints
- Ensure adequate calcium and Vitamin D intake through diet
Physiotherapy may be recommended after cast removal for:
- Stiffness following prolonged immobilisation
- Muscle wasting in the affected limb
- Balance and proprioception retraining after lower limb fractures
Most children return to full activity within 4–12 weeks, and the vast majority recover with no long-term complications.
8. Prevention Tips for Parents
As a Paediatrics Orthopaedics doctor in Bhubaneswar, I believe prevention is always better than treatment. Here are practical steps to reduce fracture risk in your child:
✅ Ensure adequate Calcium and Vitamin D: Milk, dairy products, green leafy vegetables, eggs, and safe sun exposure are essential for strong bones in growing children.
✅ Invest in protective gear: Helmets, knee pads, wrist guards, and elbow pads during cycling, skating, and contact sports dramatically reduce fracture risk.
✅ Create a safe home environment: Use stair gates for toddlers. Ensure bunk beds have safety rails. Remove loose rugs that cause slips.
✅ Supervised playground time: Monkey bars, climbing frames, and trampolines account for a large proportion of paediatric fractures. Supervision and age-appropriate equipment matter.
✅ Encourage weight-bearing exercise: Activities like running, jumping, and dancing help build bone density in children — making bones stronger and more resilient.
✅ Screen for Vitamin D deficiency: Many children in India — including in Odisha — are found to be Vitamin D deficient. I routinely screen for this during annual wellness visits.
✅ Do not delay after an injury: A fracture diagnosed and treated promptly heals far better than one that is walked on for days before being assessed.
9. When to Visit a Paediatrics Orthopaedics Doctor in Bhubaneswar
Please bring your child to see me or visit the nearest emergency facility immediately if:
🚨 There is visible bone deformity or an open wound near the injury
🚨 Your child refuses to use the affected limb at all
🚨 There is numbness, tingling, or the limb appears pale or cold (possible vascular injury)
🚨 Severe swelling develops within minutes of the injury
🚨 Your child is in uncontrollable pain
🚨 You heard a pop or snap at the time of injury
Book a consultation with Dr. Dibya Ranjan Sahoo, Paediatrics Orthopaedics doctor in Bhubaneswar, for any bone injury concern, growth plate evaluation, or follow-up after a fracture. Early assessment leads to better outcomes — always.
Frequently Asked Questions (FAQ)
Q1. How do I know if my child has a fracture or just a sprain?
A fracture and a sprain can sometimes feel similar immediately after injury. However, signs that suggest a fracture include: severe localised pain, visible deformity, rapid swelling, inability to use the limb, and tenderness directly over the bone rather than over soft tissue. The only definitive way to confirm is an X-ray. If in doubt, always visit a Paediatrics Orthopaedics doctor in Bhubaneswar or the nearest emergency facility.
Q2. What is a greenstick fracture in children?
A greenstick fracture is a type of fracture unique to children. Because young bones are more flexible than adult bones, they can bend and crack on one side without breaking completely — similar to how a young green twig bends rather than snaps. These are most commonly seen in the forearm and are typically treated with a cast. Most children recover fully within 4–6 weeks.
Q3. How long does it take for a child’s bone to heal after a fracture?
Children heal bones significantly faster than adults. A simple fracture in a toddler may heal in 2–3 weeks. For school-age children, most fractures heal in 3–6 weeks. Adolescents may take 4–8 weeks. Complex fractures, growth plate injuries, or surgical cases may take 6–12 weeks. Your treating doctor will confirm healing through follow-up X-rays before returning to full activity.
Q4. What is a growth plate fracture and why is it concerning?
The growth plate (physis) is the area of developing cartilage near the ends of long bones where a child’s bone grows longer. It is structurally weaker than mature bone and is a common fracture site in children. If a growth plate fracture is not managed correctly, it can disrupt normal bone growth — resulting in one limb being shorter or a deformity developing over time. About 15–30% of childhood fractures involve the growth plate, making specialist evaluation essential for all joint injuries in children.
Q5. Does my child need surgery for a fracture?
Most paediatric fractures treatment — approximately 70–80% of cases — does not require surgery. Children’s bones heal well with casting or splinting. Surgery is considered for displaced fractures that cannot be held in correct alignment with a cast, open fractures, significant growth plate injuries, or fractures involving a joint surface. Dr. Dibya Ranjan Sahoo will discuss all options with you and recommend the most appropriate, least invasive approach for your child’s specific fracture.
Q6. Can my child play sports after recovering from a fracture?
Yes, in the vast majority of cases, children return to full sporting activity after a fracture heals completely. However, it is essential to wait until the bone is fully healed (confirmed on X-ray or clinical examination) and any required physiotherapy is completed. Returning too early significantly increases the risk of re-fracture. Your Paediatrics Orthopaedics doctor in Bhubaneswar will advise a safe return-to-activity timeline specific to your child’s fracture.
Q7. How can I prevent fractures in my child?
Key prevention strategies include ensuring adequate calcium and Vitamin D intake, using protective gear during sports and cycling, supervising play on climbing equipment, creating a safe home environment, and screening for Vitamin D deficiency — which is common in Indian children. Encouraging weight-bearing physical activity also builds bone density and reduces long-term fracture risk.
Conclusion
Paediatric fractures are common, but with the right knowledge and timely medical care, the vast majority of children recover completely and return to their active lives. The key is recognising the signs early, seeking evaluation without delay, and trusting a specialist who understands the unique demands of a growing skeleton.
If your child has sustained a bone injury — or if you simply want to discuss their bone health — I welcome you to book an appointment at my clinic. As a dedicated Paediatrics Orthopaedics doctor in Bhubaneswar, my goal is to give every child the most appropriate, evidence-based care so they can heal quickly and grow well.
Dr. Dibya Ranjan Sahoo Paediatrics Orthopaedics Doctor in Bhubaneswar,UTKAL ORTHO CARE, Pragati Enclave, MIG S 21, Niladri Vihar, Chandrasekharpur, Bhubaneswar, Odisha 751016 📞083288 83481 🌐 https://drdibyaranjansahoo.com
Disclaimer: This article is for educational purposes only. It does not substitute professional medical advice, diagnosis, or treatment. Always consult a qualified Paediatrics Orthopaedics doctor for any medical concern regarding your child.